

By Marty Lerner, Ph.D.
Board member
Bulimia, anorexia, binge eating, and Food Addiction all involve either an acquired or pre-existing [sometimes genetic] dysfunction of the reward system in the brain. The phenomena of craving, compulsion, obsessive rumination about a substance, and so on are all biological as well as psychologically driven. Much of the research confirms this. Today, we are viewing the human brain in real-time and bearing witness to the neural reward pathways of addictive substances as they are introduced into the bodies of volunteers. Indeed, a graphic display of these differences between a Food Addict and their non-addict peers has been demonstrated repeatedly within the peer-reviewed medical literature.
This means that the more a person eats the foods they are addicted to, the stronger their cravings for those foods become. This is due to chemical processes going on in the brain. These chemical processes change the brain in a way that reinforces cravings and interfere with clear thinking, impulse control, and decision-making. Worse, tolerance [needing more to achieve the same effect] increases, making it harder to abstain from the food or foods you are addicted to. The cravings associated with addiction are so intense and thinking is so impeded that psychological therapy and other kinds of training in how to cope with feelings tend to be much less effective, or ineffective, if used exclusively. Therefore, trying to teach someone with Food Addiction to eat their trigger foods moderately is almost always unsuccessful. Moderation is not the appropriate treatment for Food Addiction. When moderation is prescribed to the Food Addict, it can cause harm and needless suffering.
Despite petitions to the World Health Organization and the American Psychiatric Association urging the inclusion of food as a substance use disorder, consider the following line of reasoning to clarify the spirit of those arguments:
The “naysayers:” Drug addiction, alcohol dependency, and process addictions [e.g., compulsive gambling] are substances and behaviors that are not necessary for life. Food is.
The “believers:” But so is water and air. However, people do not consume water & air beyond their biological needs or in ways that threaten their survival. So perhaps the problem is semantics:
“Drug addiction” does not say that all drugs are addictive.
“Food Addiction” does not say that all foods are addictive.
So, does that mean “emotional eating” doesn’t play a part in all this? The fact is we do not know how much of a Food Addict’s cravings are triggered solely by “addictive foods” or how much emotional triggers drive the compulsion. Is it “either/or” as opposed to some combination of the two?
Here’s a way of looking at the difference between an eating disorder [such as anorexia or bulimia] and Food Addiction.
a-Food Addiction ALMOST ALWAYS involves a need to identify and abstain from identified [offending] food substances, much like an alcoholic must abstain from alcohol and most mood-altering substances. [biological triggers]
b-Eating disorders DO NOT ALWAYS necessitate an abstinent stance from foods such as those that trigger addictive eating. At the same time, many people diagnosed with an eating disorder also experience Food Addiction as an integral driver of their ED.
c-As such, those who have a history of binge eating, binge eating and purging [bulimia], compulsive overeating, and some forms of anorexia [usually purging types] often need to identify and abstain from “trigger foods.” Hence, a combination of biological and emotional triggers tends to drive these.
“Eating disorders are typically associated with various maladaptive patterns of behavior related to food, its consumption, and the ensuing effects on a person’s emotional and physical well-being. It may, or may not, include attempts to offset the “consequences” of these behaviors by using or abusing compensatory agents and behaviors such as purging, compulsive exercising, periods of self-imposed starvation, and so on.” [M. Lerner 2010, 2024, A Guide to Eating Disorders and Food Addiction]
Given the debate as to what causes someone to develop an eating disorder, it is more likely that the answer is not a simple “one size fits all.” The mainstream professional community believes the answers are hidden within the emotional psyche of the sufferer. Whether anorexic, bulimic, or a binge eater, the persistence of self-medicating vis-à-vis overeating, starving, or purging is thought to be a misguided attempt to control unwanted emotions or, in many cases, avoid the pain of experiencing past, present, or future trauma. This belief attributes disordered eating as an attempt at regulating emotions regardless of their origins.
A growing number of professionals, myself among them, believe the biological piece to the puzzle has long been ignored or at best minimized. Recognizing how both emotional and biological factors interact to drive an eating disorder is tantamount to successful treatment. Although recovery from an eating disorder is possible by learning to better manage a particular issue or stressors – namely by “resolving” the emotional trigger[s], it is also possible that such recovery will be short-lived. In other words, this same person may have only solved half or a quarter of the problem, and the physical piece [reactivity to trigger foods] needs to be identified and eliminated to achieve long-term recovery. One might consider addressing both until science finds a reliable means to determine this. Stated another way, if years of “therapy” yield a short-lived remission, look to the food or biological remedy. If adherence to a food plan devoid of probable trigger foods yields little progress, consider the emotional baggage that must be addressed. In either case, the answer will present itself if one keeps an open mind.
People who treat both eating disorders and Food Addiction and are well-versed in the addiction field will tell you both disorders exist for a majority of their clients, with varying proportions at various times. This is what makes treating Food Addiction and related food/eating disorders so complex and so challenging.
As is often the case when both conditions are present, chemical dependency on food substances [or mood-altering effects of dieting and starvation] usually interferes with a person’s judgment and self-control. Much like treating any form of addiction, abstinence from the offending substance[s] would seem logical. There are two caveats: abstinence is the beginning of long-term recovery, not the end game. Space is likely needed for “harm reduction” when considering the expectations for progress and a good outcome — perfection with any food plan can be counterproductive and contribute to “all or none thinking.” Hence, a simple way to think of harm reduction is to strive for progress toward the ideal yet plan for contingencies. In other words, minimize harm by decreasing the frequency, amount, and duration of any unplanned lapses or minor deviations back into ED behaviors or trigger foods. In time, the eating disorder behaviors may stop despite the occasional imperfections around the prescribed food plan.
Food Addiction might well be thought of as a substance use disorder, with the substance being individually identified food substances such as sugar, salt, certain fats, highly processed foods, and so on. Much like other substance use disorders, the substances may vary from alcohol to narcotics to behavioral addictions such as gambling and sex.
Eating disorders might be considered an umbrella from which Food Addiction, as well as related eating disorders, may be grouped together or separately defined. Almost without exception, identification and complete abstention from certain food substances are a prerequisite to overcoming Food Addiction. As noted, this might not ALWAYS be the case with some individuals harboring an eating disorder diagnosis or history. However, most abstinent food plans are at least healthy and serve as part of an ongoing recovery lifestyle. What are often called “abstinent food plans” typically consist of more nutritious whole foods, eliminating ultra-processed foods and ensuring reasonable and healthy amounts of these foods.
Many people who fit the medical criteria for binge eating disorder, bulimia, and/or specific variants of anorexia also appear to fit the description of a Food Addict. How much and how many Food Addicts manifest an eating disorder, or what I would consider “dually diagnosed,” may be a subject for future study.
By analogy, some alcoholics also are dually addicted and can be identified as “addicts and alcoholics.” Some Food Addicts may well be recognized as a “bulimic and a Food Addict.” To be clear, the concept is more important than the limits set forth with language and semantics. The implications are a matter of securing effective treatment.
Marty Lerner, PhD., is the founder and CEO of Milestones In Recovery, located in Cooper City, Fla. MilestonesProgram.Org He is a member of the Food Addiction Institute board of directors.
A primary goal of the Food Addiction Institute is to foster recognition of food as a substance use disorder by the American Psychiatric Association and the World Health Organization. We have many reasons for this, but one is that without a diagnostic code, many health professionals will not screen for it.
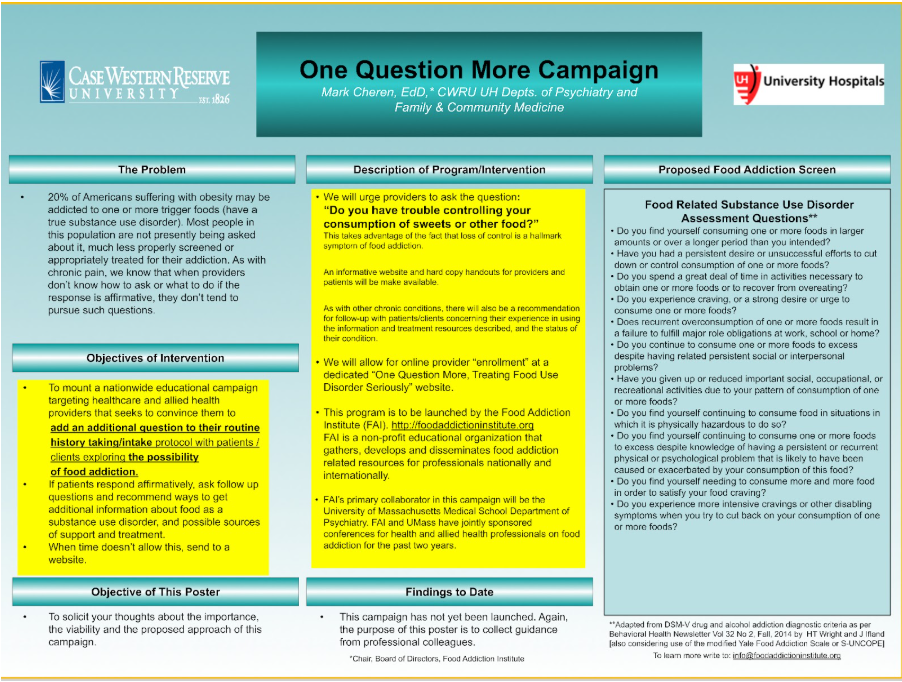
Allies of the institute are already engaged with those institutions on winning recognition. But the institute believes enough evidence for one or more food-related substance use disorders already exists to urge health care professionals to add one more question to their intake protocol: “Do you have trouble controlling your weight, eating, and/or consumption of sweets and other food?”
Loss of control is one of 11 criteria for a substance use disorder in the Diagnostic and Statistical Manual of the American Psychiatric Association. Its presence does not, by itself, trigger a diagnosis. Two or three indicate a mild disorder, four or five indicate a moderate disorder, and any more signify a severe disorder.
But you can’t get to two without one, so it’s a place to start. For patients who answer affirmatively, consider these follow-up questions, adapted from DSM-V drug and alcohol addiction diagnostic criteria as per Behavioral Health Newsletter Vol 32 No 2, Fall, 2014 by HT Wright and J Ifland:
But you can’t get to two without one, so it’s a place to start. For patients who answer affirmatively, consider these follow-up questions, adapted from DSM-V drug and alcohol addiction diagnostic criteria as per Behavioral Health Newsletter Vol 32 No 2, Fall, 2014 by HT Wright and J Ifland:
Beginning to look for such symptoms is key because, very conservatively stated, scores of millions in the world experience Food Addiction, and the vast majority don’t know it. How can patients seek appropriate treatment, or even consider appropriate treatment, without knowing the nature of their illness?
Nutritionists who believe in Food Addiction are vital resources for real and potential Food Addicts. Some of them are key allies of the institute, but they and others like them are not in the mainstream.
One reason for this, especially among registered dietitians, is that they feared they could even lose their credentials or be otherwise marginalized for their beliefs about Food Addiction. They have been courageous to follow their education and instincts to recognize Food Addiction when present in clients, and to counsel them appropriately.
An initiative of the institute, conceived by board member H. Theresa Wright, MS, RD, LDN, is to host what amounts to a support group for nutritionists and dietitians who treat Food Addicts. The group goals are to bolster experienced nutritionists who may have felt marginalized, to help younger practitioners build and expand practices so that more Food Addicts may be helped, and for all to share perspectives and best practices.
If you are a nutritionist or dietitian who’d like to join, please reach out to us. If you know a professional who might be interested, please share this information.